This article has been reviewed for clinical accuracy by Dr. Rachel Armstrong
If you’ve had thoughts like, “My baby would be better off without me,” you’re not alone. But those thoughts do not define who you are.
Pregnancy and new parenthood are often described as joyful milestones. While they certainly can be, they can also bring enormous emotional, physical, and psychological changes. Many new or expecting parents experience anxiety, self-doubt, sadness, or overwhelming stress during this time.
For some, those struggles become something more.

Persistent self-critical thoughts can spiral into feelings of hopelessness, self-harm, or suicidal thoughts. These experiences can feel frightening and isolating, leading many people to believe they must be “bad parents” or that something is fundamentally wrong with them.
The reality is much different.
Mental health professionals increasingly recognize that one important contributor to suicidal thoughts during pregnancy and after childbirth is rumination, a pattern of repetitive, self-critical thinking that can gradually deepen emotional distress. Understanding rumination can help explain why these thoughts develop and, more importantly, why effective treatment is available.
Most people don’t use the word rumination to describe what they’re experiencing.
Instead, they say things like:
These are all common ways people describe rumination.
Dr. Sheila Crowell defines rumination as, “recurrent dwelling on feelings, problems, upsetting events, and negative aspects of the self.”
Unlike productive problem-solving, rumination rarely leads to solutions. Instead, the same worries and self-criticisms replay repeatedly, making it increasingly difficult to step back from them.
Pregnancy and the postpartum period involve enormous life changes. As Dr. Crowell explains, there is simply a great deal to think about during this stage of life.
People may find themselves worrying about:
Many of these concerns are completely understandable. The challenge is that when those worries become repetitive and self-critical, they can begin feeding emotional distress instead of helping us solve problems.
One of the most important ideas that Dr. Crowell discusses is that suicidal thoughts often do not appear suddenly.
Instead, repetitive negative thinking can slowly become more painful over time.
She explains that repetitive, passive, self-critical thoughts can eventually escalate into thoughts such as:
These thoughts can be deeply frightening. Many parents immediately assume that having them means they are dangerous, broken, or failing. In reality, these thoughts often reflect overwhelming emotional pain, not a person’s character or love for their child.
Rumination often involves comparing ourselves to an impossible standard.
Parents may find themselves thinking:
As these comparisons repeat over and over, they begin to shape how a person feels about themselves. Instead of seeing one difficult moment, the mind starts building a much broader conclusion: “I’m not good enough.”
Unfortunately, rumination doesn’t simply replay painful thoughts… it often intensifies them.
One of the most reassuring parts of Dr. Crowell’s discussion is her explanation that rumination often becomes a habit.
She compares it to nail biting: Many people don’t notice they’re biting their nails until they’ve already been doing it for several moments.
Rumination works similarly.
People often don’t notice they’re spiraling until they suddenly realize they’re in a terrible mood or thinking something shocking about themselves.
Dr. Crowell explains that many people don’t recognize what has been happening until they catch themselves thinking something like: “I’d be better off dead.”
By that point, the spiral has often been building for quite some time. Recognizing these patterns is not about blaming yourself. It’s about learning to notice the spiral earlier.
Rumination doesn’t only affect your thoughts. It often affects your body as well. Some people notice:
These physical sensations can become warning signs that your mind has entered a rumination cycle. Learning to recognize them early can make it easier to interrupt the pattern before it grows stronger.
One reason rumination is so difficult is that it creates the illusion of productivity. It feels like you’re working through a problem. In reality, Dr. Crowell explains that rumination often functions as a form of avoidance. Instead of helping people move forward, it can lead them to:
Unfortunately, isolation often gives rumination even more room to grow.
Research examining postpartum self-injurious thoughts and behaviors among Utah mothers show some interesting findings. Several factors were associated with greater risk, including:
When researchers looked at these factors together, two stood out most strongly:
The encouraging news is that rumination can be treated.
One approach Dr. Crowell discussed is Rumination-Focused Cognitive Behavioral Therapy (RF-CBT). Rather than telling people to “just stop worrying,” this approach helps them first become aware of the thoughts that have been running automatically in the background.
Many people are surprised by what they discover. Dr. Crowell notes that clients often say things like: “I can’t believe I say those things to myself.” or “I would have never said something like that to someone else.”
That awareness becomes the starting point for change.
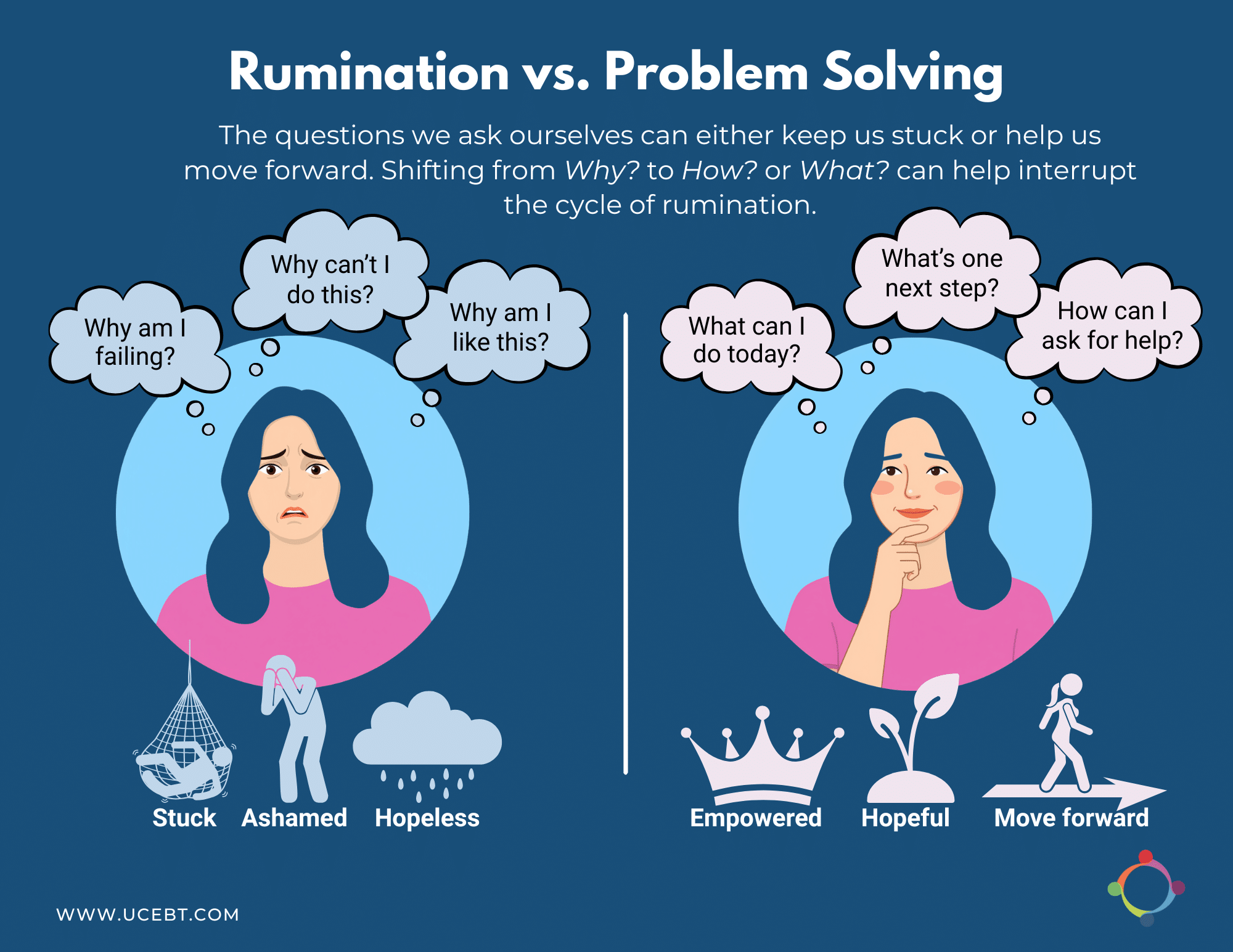
One particularly powerful strategy discussed in the presentation involves changing the kinds of questions we ask ourselves.
Rumination often sounds like:
These “why” questions tend to leave people feeling stuck, hopeless, and ashamed.
Instead, therapy encourages more concrete questions, such as:
Dr. Crowell explains that people often notice a remarkable difference in how these questions feel. The “why” questions create hopelessness. The “how” questions begin creating a path forward.
Another important part of treatment involves learning to recognize compassionate thoughts that already exist.
Rather than replacing negative thoughts with unrealistic positivity, Dr. Crowell encourages people to develop statements they genuinely believe.
For example, instead of saying, “I’m the world’s best parent,” a more compassionate statement might be, “I may not always be perfect, but I’m really trying, and my kids can tell.”
Many people discover they already have compassionate thoughts, they’ve simply been drowned out by rumination.
If you’re experiencing thoughts of harming yourself, or believing your loved ones would be better off without you, those thoughts deserve compassionate attention.
They are not something you have to carry alone. Dr. Crowell also discussed the role of Dialectical Behavior Therapy (DBT), an evidence-based treatment designed to reduce emotion dysregulation and suicidal behaviors. She noted that crisis response plans and specialized treatment can be extremely helpful for people experiencing suicidality during pregnancy or the postpartum period.
Seeking help is not a sign that you’re failing. It’s a sign that you’re responding to emotional pain with courage.
Pregnancy and parenthood are times of tremendous change. If you’ve found yourself spiraling into self-criticism, hopelessness, or thoughts that frighten you, know that these experiences are treatable.
You are not weak. You are not alone. And you are not defined by your thoughts.
At UCEBT, our clinicians provide evidence-based treatment for perinatal mental health concerns, including depression, anxiety, obsessive-compulsive disorder, trauma, and other emotional challenges that can arise during pregnancy and the postpartum period. With the right support, it is possible to interrupt the cycle of rumination, reduce emotional suffering, and begin moving toward healing.

Dr. Rachel Armstrong obtained her doctorate from William James College in Boston, MA. She received training and clinical experience in behavioral health interventions and health psychology, including training in clinical hypnosis for IBS, biofeedback assisted relaxation training, and behavioral medicine interventions. She completed her APA-accredited internship at LifeStance Health where she gained experience working in integrated behavioral health settings. Currently, Dr. Armstrong is a postdoctoral fellow at UCEBT.
Perinatal mental health conditions are common, treatable, and nothing to be ashamed of. Our therapists are here to help you find relief and begin healing.
